EndoAxis Clinical Team

In the world of hormones, we are often overwhelmed by options for treatment. We all find our niches and preferences, and it is wise practice to know all the options as well as alternatives, risks/benefits to each therapy.
It is also equally important to understand our expectations for treatment and evaluation of hormone treatment efficacy. We need to understand the why of testing: what are we looking for? Understanding the chosen therapy enhances our capacity for treatment and effective testing evaluation.
As an addition to your provider tool kit, here is a review of the different types of hormone therapies, as well as their relevance on DUTCH testing. This is vital for understanding hormone supplementation, interpretation, and overall effective treatment.
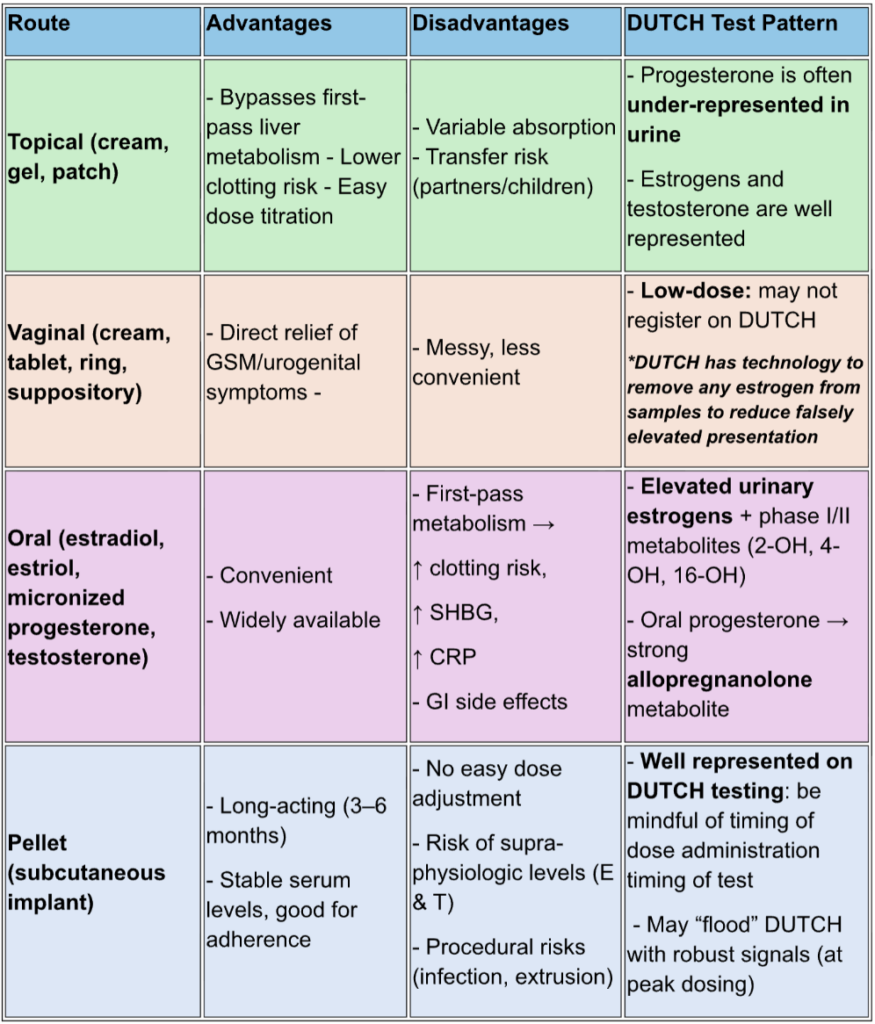
Topical
(transdermal creams/gels/patches)
Advantages
- Bypasses first-pass liver metabolism which means more stable estradiol levels.
- Lower clotting risk compared to oral (due to bypass of the liver).
- Can be titrated easily by dose adjustments.
Disadvantages
- Variable absorption (skin thickness, melanin concentration, fat distribution, application site).
- Potential for transfer to partners/children more so with creams and gels vs the patch.
DUTCH Impact
- Topical progesterone: shows up as lower urinary levels than expected, because topicals don’t always metabolize in the same way as oral/vaginal routes. You may see clinical effects but only modest metabolites. This can create confusion if a clinician only interprets the test at face value.
- Topical estrogens and testosterone: these are well represented on urinary testing and offer wonderful insight into dosing alongside symptom evaluation.
Vaginal
(creams, tablets, rings)
Advantages
- Excellent direct local effect (excellent for urogenital symptoms, GSM).
- Minimal systemic absorption at low doses, which may be a safer option in the long-term for some women (ie – high risk).
- Robust vaginal dosing shows supportive systemic absorption. You can still achieve systemic response with vaginal application (1).
Disadvantages
- Some women do not prefer vaginal routes of administration.
- Can be messy or inconvenient.
DUTCH Impact
- DUTCH testing specifically uses a technology to allow for accurate representation of vaginal hormone dosing.
Oral
(estradiol, estriol, micronized progesterone, testosterone)
Advantages
- Convenient, widely available.
- Usually higher compliance.
Disadvantages
- Undergoes first-pass metabolism in the liver which may lead to a higher stimulation of clotting factors, SHBG, CRP.
- More GI side effects.
- Less “bioidentical” effect on tissue compared to transdermal: for example, due to liver metabolism and breakdown, a 100 mg dose of Prometrium will generally result in tissue effect of around 50 mg. This should be taken into consideration with choosing the dose of Oral Micronized Progesterone (OMP).
DUTCH Impact
- Much higher urinary estrogen levels and metabolites due to liver conversion. You’ll see elevated phase I and II metabolites (2-OH, 4-OH, 16-OH pathways) compared to the same systemic dose of topical.
- Oral progesterone → may see high metabolites; though DUTCH testing has ranges that are adjusted for consideration of oral progesterone supplementation.
Pellets
(subcutaneous implants)
Advantages
- Long-acting, convenient (3–6 months).
- Stable serum levels (avoids compliance issues).
Disadvantages
- Difficult to adjust dose once placed.
- Risk of supra-physiologic levels → androgen excess, high estrogen, aromatization.
- Insertion procedure risks (infection, extrusion).
DUTCH Impact
- Pellet therapy is well represented on DUTCH testing. It is important to keep in mind the timing of testing (peak, average, trough).
- At peak testing, DUTCH typically shows very robust metabolite patterns because continuous exposure drives metabolism down all pathways. You may see “flooded” estrogen metabolites, or high androgens with strong downstream conversion to estrogens (via aromatase).
Delivery Route & DUTCH Impact
Delivery route doesn’t just affect hormone levels—it shapes how hormones look on a DUTCH test.
- Oral = heavy liver metabolism → high metabolites.
- Topical = well represented on DUTCH testing for estrogen and testosterone. Progesterone shows “underwhelming” urine results.
- Vaginal = well represented due to DUTCH technology, OR may be over-represented.
- Pellets = well represented on DUTCH testing. At peak testing, metabolite flooding will likely show, sometimes masking the subtleties of pathway balance.
Clinical Pearl
DUTCH testing doesn’t just reflect dose—it reflects delivery method, metabolism, and tissue exposure.
Understanding the different therapies and how they show up on urinary testing greatly impacts:
- Why we test.
- Our direction forward for treatment.
EndoAxis’ superior technology takes these DUTCH ranges into consideration: not just the parent hormone value – it considers the full picture of patterns through metabolite and enzyme recognition.
The EndoAxis report goes beyond the expected hormone presentation. It welcomes you to a world of in-depth interpretation with supportive explanation and valuable insight for understanding how to empower you as a provider in offering the most powerful treatment options available.
Don’t have the link to be part of this movement? Join us now and get on board for stellar provider education and enhanced patient care!
